Acute Symptomatic Seizures
- Previously termed "provoked seizures"
- Seizures that occur in close temporal relation to an acute CNS insult
- metabolic, toxic
- structural
- infectious
- inflammatory
- How long is acute?
- for cerebrovascular, traumatic, or infectious causes - symptomatic if they precede the seizure by <7 days
- may be longer in some cases - e.g. continuing evidence of active CNS infection
- for metabolic disturbances - within 24 hours of the laboratory abnormality
- for alcohol withdrawal - within 7-48 hours
- based on epidemiological operational definitions - and hence completely arbitrary!
- consider suspected seizure precipitants in the context of each patient
Epidemiology
- Classic study of Annegers and Hauser of newly-incident seizures in Rochester, MN
- Most commmon causes of acute symptomatic seizures:
- head trauma
- cerebrovascular disease
- CNS infection
- alcohol withdrawal
- Causes varied among age groups:
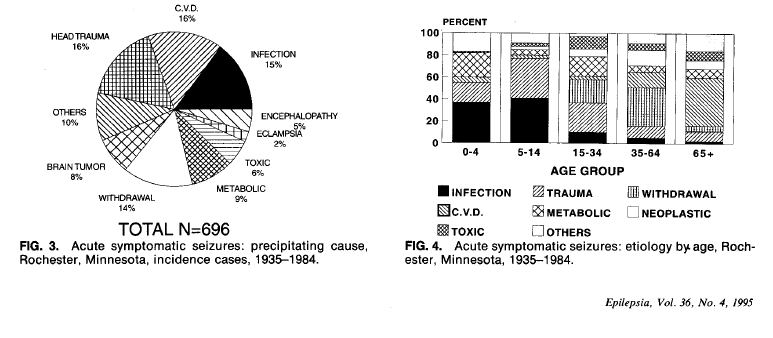
- ...with CNS infection more prevalent in childhood, and cerebrovascular disease more prevalent among the elderly
Traumatic Brain Injury
- Risk of seizure after TBI depends on severity of injury and time since the injury
- Even "mild" TBI (LOC or post-traumatic amnesia <30 min, no skull fracture) increases risk
- Cohort of 4541 post-TBI patients (Annegers 1998)
- 117 early seizures (<1 week from injury, or <1 month for injuries with protracted course), one third of the cases were mild TBI
- Early seizures are probably due to direct neuronal injury, late seizures due to gliotic scarring
Cerebrovascular Disease
- Overall risk of post-stroke seizure is 4-10% (includes acute and remote symptomatic seizures)
- When seizures do occur, they are often in the acute-post stroke period (Bladin 2000)
- 40% of ischemic stroke patients who seized did so in the first 24 hours
- 57% of hemorrhagic stroke patients had their first post-stroke seizure in <24 hours
- Early seizures are probably due to direct neuronal injury, late seizures due to gliotic scarring (as for TBI)
CNS infection
- A clear risk factor for both acute and remote symptomatic seizures
- Seizures occurred in 19% of survivors of encephalitis or meningitis during the acute phase of infection (Annegers 1998)
- AAN practice parameter recommends LP for febrile patients presenting with seizure (Krumholz 2007)
Drugs
- Always review the medication history carefully...
- applies to both prescribed and non-prescribed (OTC or "recreational") drugs
- a collateral historian or repeated questioning may be necessary
- Drugs of Abuse
- Alcohol
- Withdrawal seizures present as a single seizure or cluster of seizures, usually 6-48 hours after cessation of heavy drinking
- "His EtOH level is negative so I didn't think the seizure was caused by his drinking..."
- Alcohol withdrawal seizures usually occur when blood alcohol levels reach zero
- A relative withdrawal state caused by temporary drop in levels may produce a seizure in an intoxicated alcohol-dependent patient
- various validated screening tools exist to screen alcohol use: CAGE, FAST, AUDIT-C, etc
- Psychostimulants
- Cocaine
- One of the most epileptogenic drugs of abuse
- Seizures occur within hours of use
- Amphetamines and MDMA (Ecstasy)
- Marijuana
- Marijuana use may increase, reduce, or have no effect on the risk of seizures - literature is not conclusive
- Some synthetic cannabinoids ("spice", "K2", "kronic")have been associated with seizures
- Heroin
- Seizures are infrequently reported with heroin use, even in overdose
- Heroin withdrawal does not cause seizures (except in neonates) - if seizures occur in this state, look for another cause
- Prescription Medications
- Opioids
- pethidine, diamorphine, methadone, propxyphene, meperdine, morphine, fetanyl, tramadol... have been implicated as the cause of seizures
- meperidine is a special case due to accumulation of its epileptogenic metabolite (normeperidine), especially in renal failure
- Antibiotics
- β-lactam antibiotics are the classic epileptogenic prescription drug
- Seizures most frequently associated with the penicillins, the cephalosporins, and imipenem
- Risk of seizure appears to depend on increasing CNS concentration, explaining the known risk factors:
- impaired renal function
- intravenous high doses
- direct CNS administration (intrathecal, intraventricular, intracisternal)
- compromised BBB (meningitis, bacterial endocarditis, sepsis, cardio-pulomonary bypass)
- Sedative-Hypnotics
- Abrupt cessation produces a withdrawal syndrome similar to alcohol withdrawal
- Withdrawal associated with barbiturates, benzodiazepines, meprobamate, chloral hydrate, zolpidem, zopiclone
- Risk of withdrwawl seizures is dose-related - they are less likely to occur when drug is taken at therapeutic doses
- Antidepressants
- Frequently named as a cause of seizures
- Real risk is probably lower:
- Tricyclic antidepressants (TCAs) probably highest risk (estimated ranges 0.4% to 1-2%
- Monoamine oxidase inhibitors (MAOIs) not considered a significant risk at therapeutic doses, rarely reported to cause seizures in overdose
- SSRIs are a rare cause of seizures, even in acute overdose
- Risk of seizure with bupropion (Wellbutrin) rises above 1% for doses >450 mg/d
- As always - risk is dose-dependent, and not significant at therapeutic ranges
Medical Comorbidities
- Hepatic disease
- Renal disease
- Acute fluid and electrolyte shifts associated with dialysis
- Dialysis dysequilibrium syndrome (uncommon, seen after a first hemodialysis treatment)
- Late-stage uremic encephalopathy
- Dialysis dementia (previously caused by aluminum compounds in dialysate solutions)
- Diabetes Mellitus
- Hypoglycemic seizures
- Hyperosmolar hyperglycemic state
- Diabetic ketoacidosis
- Posterior Reversible Encephalopathy Syndrome (PRES)
- Seizures are the most common clinical feature of PRES (along with encephalopathy and headache)
- Seizure occur early in the course, and may be the presenting symptoms of PRES
- Consider PRES when risk factors are present:
- Hypertension
- Renal disease
- Lupus
- Immunosuppresive drugs (tacrolimus, sirolimus, etc)
Evaluation
- Recommendations from the AAN Practice Parameter, "Evaluating an apparent unprovoked first seizure in adults" (Krumholz 2007)
- "The history, physical, and neurologic examination are acknowledged by expert consensus to be required for the initial diagnosis and classification of seizures."
- Physical examination (table)
- Should an EEG be routinely ordered in adult presenting with an apparent unprovoked seizure?
- "The EEG should be considered as part of the neurodiagnostic evaluation of the adult with an apparent unprovoked first seizure because it has a substantial yield"
- "The EEG... has value in determining the risk for seizure recurrence"
- So should we order EEGs for apparent provoked seizures?
- I would argue no, as it is unlikely to contribute to the diagnostic yield, and the prognosis of recurrence is largely based on the etiology causing the seizures
- Should a brain imaging study (CT or MRI) be routinely ordered in an adult presenting with an appraent unprovoked first seizure?
- "Brain imaging using CT or MRI should be considred as part of the neurodiagnostic evaluation of adults presenting with an apparent unprovoked first seizure"
- This clearly applies to provoked seizures, too
- Should blood counts, blood glucose, and electrolyte panels be routinely ordered in an adult with an apparent unprovoked first seizure?
- "In the adult initially presenting with an apparent unprovoked first seizure, blood glucose, blood counts, and electrolyte panels (particularly sodium) may be helpful in specific clinical circumstances, but there are insufficient data to support or refute routine recommendation of any of these laboratory tests"
- ...obviously this recommendation does not apply in the case of suspected acute symptomatic seizures
- The reviewers who made the above recommendation excluded studies of patients presenting with obvious acute symptomatic seizures, and so the likelihood of routine blood tests discovering a significant abnormality is probably greater among acute symptomatic seizure patients
- Should a lumbar puncture be routinely performed in an adult presenting with an apparent unprovoked first seizure?
- "In the adult initially presenting with an apparent unprovoked first seizure, lumbar puncture may be helpful in specific clinical circumstances, such as patients who are febrile, but there are insufficient data to support or refute recommending routine lumbar puncture"
- Should toxicologic screening be routinely ordered in an adult presenting with an apparent unprovoked first seizure?
- "In the adult presenting with an apparent unprovoked seizure, toxicology screening may be helpful in specific clinical circumstances, but there are insufficient data to support or refute a routine recommendation for toxicology screening"
- I would suggest that a reliable collateral historian is more helpful (especially since it is not practically possible to screen for all potentially epileptogenic substances)
References
- Annegers, J. F., Hauser, W. A., Lee, J. R., & Rocca, W. A. (1995). Incidence of acute symptomatic seizures in Rochester, Minnesota, 1935-1984. Epilepsia, 36(4), 327-333.
- Karceski, S. (2014). Acute symptomatic seizures and systemic illness. Continuum (Minneapolis, Minn.), 20(3 Neurology of Systemic Disease), 614-623. doi:10.1212/01.CON.0000450969.61204.6f
- Krumholz, A., Wiebe, S., Gronseth, G., Shinnar, S., Levisohn, P., Ting, T., et al. (2007, November 20). Practice Parameter: evaluating an apparent unprovoked first seizure in adults (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. doi:10.1212/01.wnl.0000285084.93652.43
