For Physicians
Sleep disordered breathing (SBD) is a spectrum of chronic disease conditions that are united by a reduced oxygen perfusion while sleeping. Recent studies suggest 1-3% of children suffer from SBD. Severe cases of SBD are often detected early, with treatment beginning before 2 years old. However, many mild to moderate cases of SBD go undiagnosed, leaving a child with a chronic disease condition with significant impact on the systemic health and craniofacial growth.
SDB is often multi-factorial, with several etiologies or combination of problems that span across multiple disciplines. Physicians commonly acknowledge the need for ENT and respiratory management. However orthodontists should be considered key contributors as well. Children with SDB often present with specific oral and craniofacial characteristics whose treatment may improve SBD symptoms. Learning to recognize signs and symptoms of mild to moderate SBD, then knowing where to refer is critical for managing children sleep disturbances.
The most common etiology of SBD in children is adenoid and tonsil hypertrophy leading to upper airway obstruction. However, adeno-tonsillar hypertrophy is not the only cause of SBD. Any form of nasal obstruction - whether a deviated septum, chronic rhinitis, or other pathology - could lead to similar symptoms. While tonsil and adenoid hypertrophy often resolves on it's own during late adolescence, for those children with SBD the physical, psychiatric, and emotional damage is often permanent.
With the growing number of children suffering from obesity, a second form of pediatric SDB is becoming increasingly common. Obese children may present with adult-like forms of SDB commonly characterized by mandibular retrognathia and increased neck circumference.
In addition to the common primary etiologies, physicians should be familiar with, and able to identify common co-morbidities and risk factors. These conditions may work with negative synergy and co-contribute to the development or worsening of SDB. Physicians should be able to collaboratively recognize the following conditions in children suspected to have SDB:
- Asthma
- Chronic allergies
- Obesity
- Chronic environmental irritants (eg. indoor pets, parent's who smoke)
- Pre-term birth
- African decent ethnicity
Currently, the definitive diagnosis of sleep apnea for children is only available with overnight polysomnography (PSG). Similarly, the reference standard diagnosis of upper airway obstruction is flexible tube endoscopy. Rarely is a primary care physician able to provide definitive diagnosis of SBD or define its precise etiology. However PCPs do have tools at their disposal to provide accurate screening.
There are numerous questionnaires available to screen SDB. The most widely accepted for children is the Pediatric Sleep Questionnaire (PSQ). Physicians should become familiar with the questionnaire, using it both to improve and supplement their own clinical judgment.
While enlarged tonsils and adenoids are not in themselves reason for referral to an otolaryngologist, tonsil and/or adenoid hypertrophy in the presence of SBD symptoms is absolutely a valid indication for referral. In such a situation the PCP should not delay or suggest the child will outgrow the problem. While the adenoids and tonsil enlargement may spontaneously resolve, the damage done by SDB may never be reversed.
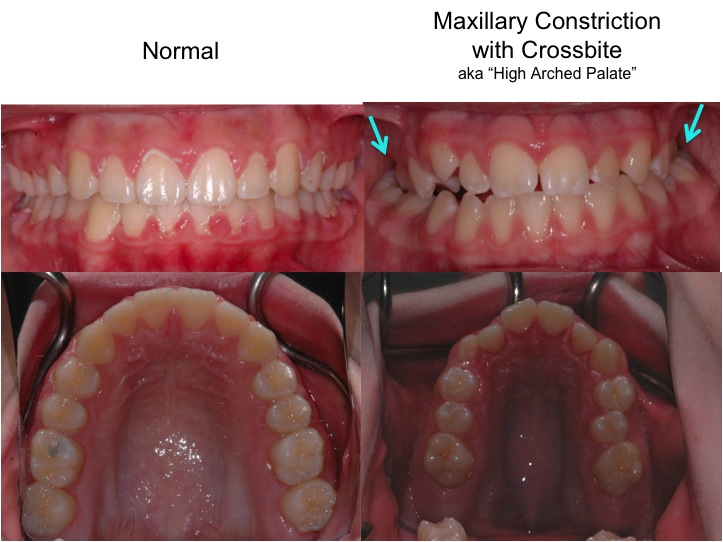
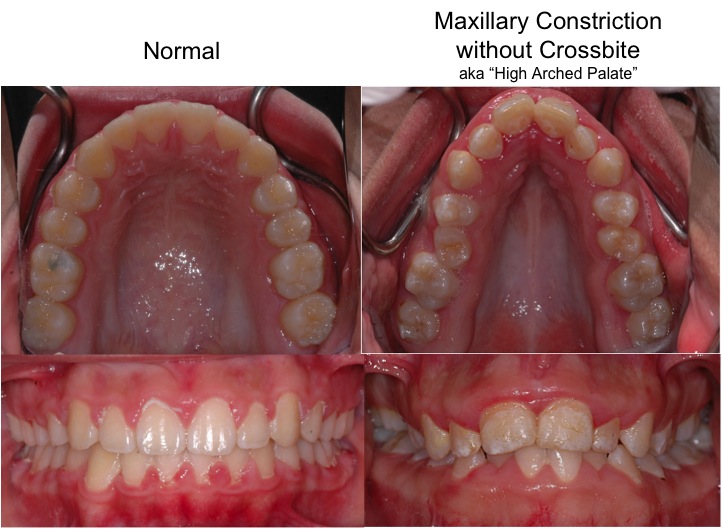
Another tool available to physicians is recognizing predictable facial characteristics of most children with SDB. Suborbital venous pooling, hypotonic peri-oral muscles, weak chin projection, and maxillary incisor teeth that appear protrusive relative to the mandibular teeth (i.e., increased overjet) are common findings. For physicians that dare to learn intra-oral anatomy, maxillary constriction often with dental crossbite is commonly observed. These are the more accurate anatomical landmarks to evaluate when looking for a "high arched palate".
Treating these craniofacial features — especially maxillary constriction and weak chin projection — can have a significantly positive effect on pediatric SDB. Therefore, in addition to the otolaryngologist and pulmonologist, the PCP should consider orthodontists as part of the referral destination for children with SDB.
SBD is often associated with specific oral and craniofacial characteristics. There is growing evidence treating these problems can be with skeletally directed orthodontic treatments might provide therapeutic benefit.
If a physician identifies a child with suspected SDB, a referral to an orthodontist is warranted if any of the following characteristics are present.
Craniofacial:
- Mandibular retrognathia
- Midface deficiency
- Vertical growth direction (aka "long face syndrome" / "adenoids faces")
{kind=link}
{kind=link}
{kind=link}
Dental / Intra-oral:
- Maxillary constriction with crossbite (aka "high arched palate")
- Maxillary constriction without crossbite (aka "high arched palate")
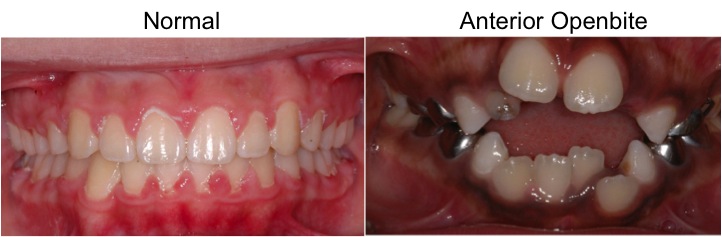
- Anterior Openbite
- Excess overjet
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rapid maxillary expansion may be one orthodontic treatment with airway benefit. For children with combined maxillary transverse constriction and hypertrophic adenoids, recent evidence suggests adenoidectomy and rapid maxillary expansion (RME) were both necessary to fully resolve symptoms. However, RME is not a "cure" for nasal obstruction. While numerous studies demonstrate improved symptoms, very rarely are complete cures observed.
Likewise evidence exists that mandibular repositioning appliances can be successful for managing SBD for children with mandibular retrognathia as the primary etiology. For these children, SBD management would be very similar to adult management of SDB for which a strong body of evidence exists.