Study Design
This is an observational study that examines the quality of transitions of frail elderly clients between and among three care settings: Nursing Homes (NHs), Emergency Medical Services (EMS), and Emergency Departments (EDs). In addition to an integrated Knowledge Translation approach, it uses multiple data sources, data collection procedures and analytic techniques.
Description
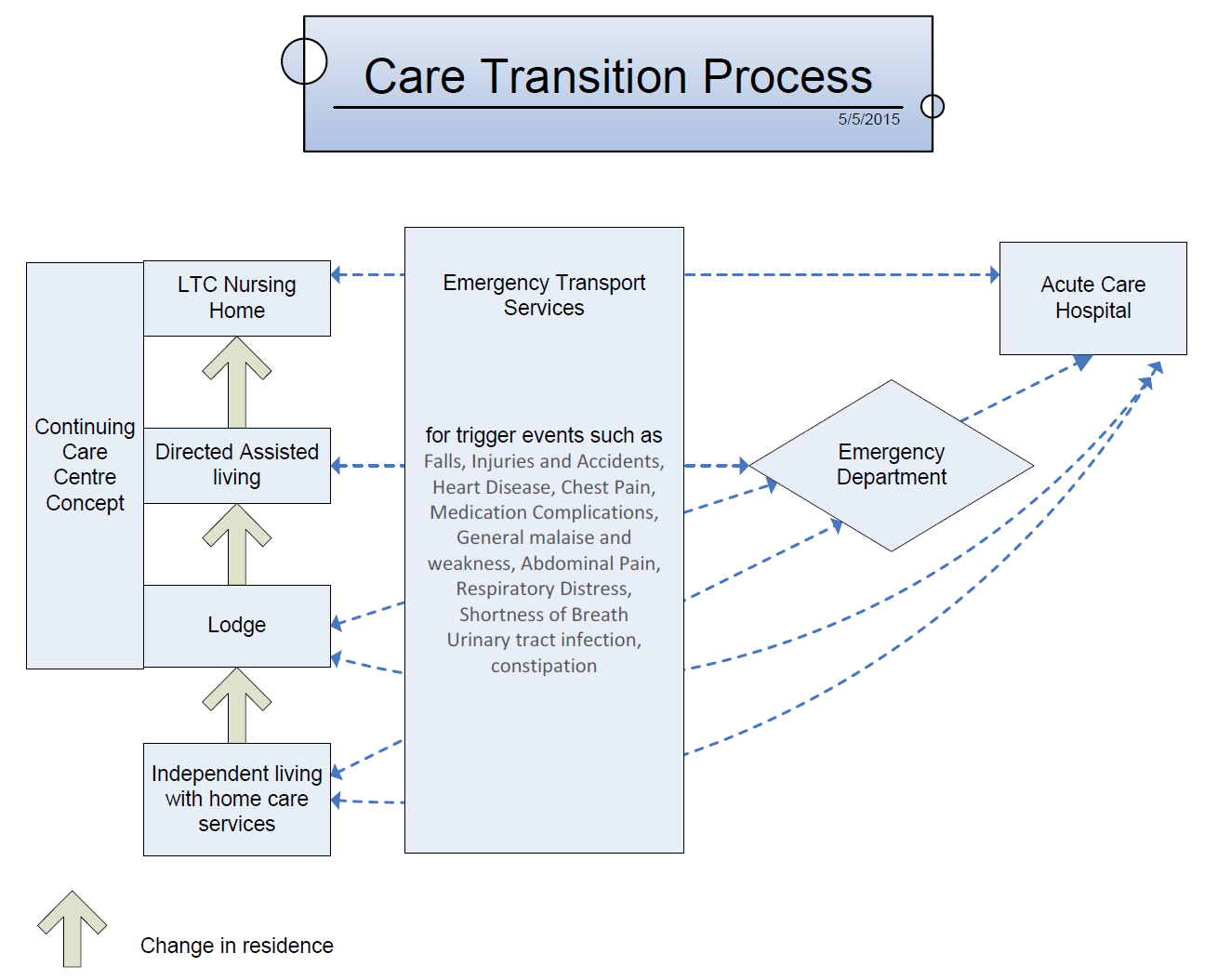
In the OPTIC Transition Process diagram, we have conceptualized the transition process that a nursing home resident experiences related to the NH and ED - the transition of interest. We have documented all relevant and important aspects of this transition process; however, to keep the project manageable and ensure we focus thoroughly on one set of dimensions, we have identified selected elements of the transition that we will not examine and represented them as black boxes in the diagram.
{kind=link}
Methods
This study will be conducted in Kelowna, BC (Central Okanagan area of the IH Region), and Edmonton, Alberta (Capital Health zone of Alberta Health Services). This is beneficial for many reasons:
- The two cities and surrounding areas present differences in size and composition. In 2006 Kelowna's population was approximately 110,000 while Edmonton's was just over 1 million. Kelowna, as a desirable retirement destination for many Canadians, has an older population which is growing even older more rapidly.
- The two regions are organized differently with regard to NH/ED transitions. In Kelowna, Kelowna General Hospital (KGH) is the sole receiving hospital for the nursing homes in the Central Okanagan and the only tertiary referral hospital in the Okanagan area, whereas in Edmonton, the University of Alberta Hospital (UAH) is one of five receiving hospitals within the city, one of 11 within the greater Edmonton region, and one of two tertiary referral hospitals. These two factors combined support the opportunity to study NH-ED transitions in two contrasting but adjacent provinces, thus enabling us to assess whether two contextually different systems offer relative advantages or disadvantages to a successful transition in care.
- IH Region has a strong desire to build long term research capacity with a researcher/decision-maker team committed to similar areas of need and interest and possesses the capacity and interest to assist them.
- This study affords an opportunity to include BC in the already strong prairie collaboration that exists in the Translating Research in Elder Care (TREC) team and to focus on health services research and care improvement for the frail elderly in western Canada.
Setting, Sample and Inclusion Criteria
We are working in three settings: NHs, EMS, and EDs, in two cities. Given the descriptive, observational nature of this study, all data collection will use purposive, convenience samples.
1. Emergency departments: The two EDs, KGH and the UAH. Research participants include all transferred nursing home residents and families, physicians, nurses and other ED staff.
2. Nursing Homes: The population consists of 52 NHs (14 in Central Okanagan and 38 in Edmonton). Forty three NHs send residents to these two EDs (all 14 in Central Okanagan and 29 in Edmonton). We will examine transfers from these 43 NHs and will do in-depth analyses on the 10 NHs with the highest referral rates to each of our study EDs, calculated as the number of transfers/number of beds per facility. Research participants: All individuals in the following groups will be eligible for study - transferred NH residents and their families, physicians, nurses, healthcare aides and care managers.
3. EMS: All 88 EMS staff (6 full time and 6 part time ambulance crews) in Kelowna and the 556 EMS and 145 Inter-hospital Transport staff in Edmonton will be eligible, as are the medical and administrative supervisors in each city. The research participants will be ambulance and/orinter-hospital transport crews, and medical and administrative supervisors in each city.
Data Sources and Measures
We will use mixed methods to collect and analyze data from both administrative and primary sources. This will enable us to build a practical tool to assess transition success incorporating input from multiple stakeholders. Multiple data sources and methods of data collection will also help us create a comprehensive picture of the situation in three different and complex environments.
Interviews
Interviewswill be used to explore different perspectives of care transition experiences in three settings (i.e., NHs, EMS, EDs). Semi-structured face-to-face interviews with three groups of stakeholders (residents and families, frontline healthcare providers, and managers/administrators) in both provinces will be employed to elicit key indicators of successfulness at both ends of the transition (NH and ED). Where feasible, we will use focus group interviews with healthcare providers within a study setting. The key indicators will be used to construct the items in the Older Persons' Transitions in Care Success (OPTICS) tool that will be applied to evaluate actual care transitions in Phase 3.
Administrative Data
We will collect administrative data that describes transfer activity in Kelowna and Edmonton for the three year period of the study similar to the background data we collected to prepare for this study. This will allow us to build a complete and accurate picture of transfer activity during the period of the study, to describe changes over time and to identify areas of highest priority for interventions.
Organizational Factors
Previous research linking organizational factors with the success or quality of the transition process signals the need for further exploration. Carter linked 1991-1993 Medicaid reimbursement data from Massachusetts with specific facility-level organizational and structural attributes and showed that nursing home case-mix and local hospital bed supply levels predicted hospitalization rates of NH residents. Boockvar and Burack, however, found no management level relationships between NHs, hospitals and the quality of transitions. To address this concern in the present study, similar organizational data will be obtained using a demographic profile form for each NH, ED, and EMS, which we will pilot and refine in Phase 1 of the study.
Inter-RAI Resident Data
The Minimum Data Set-Resident Assessment Instrument (MDS-RAI 2.0) is part of an international system intended to capture information about the health, physical, mental, and functional status of NH residents and is routinely collected in BC and AB. While these data can be used to assess and monitor quality of care for residents, in this study we will make use of them to adjust for case mix by NH. That is, we will adjust for case mix at the NH facility level for all participating NHs by including Resource Utilization Groups (RUGs) and Changes in Health, End-stage Disease and Symptoms and Signs (CHESS) scores in multivariate models. The Version III (RUG III) system has been validated in multiple settings. RUG III is a case mix classification system developed to monitor, track, and benchmark staffing and resident resource use. The data have been used to guide local and organizational decision making in regards to resource use and allocation which acts as a proxy for resident need. CHESS uses MDS-RAI 2.0 data to identify patients at risk for serious decline in health or mortality. The predictive validity of the instrument is supported by research: it predicts mortality independent of age, sex, disability, cognitive performance, and do not resuscitate orders. Each increment on the CHESS is associated with a distinct survival curve, with higher scores corresponding to a reduction in probability of survival.
CTAS (Canadian Triage and Acuity Scale)
CTASis a tool used by EMS and EDs that enables EDs to prioritize patient care requirements, and ensure that the sickest patients are seen first when ED capacity has been exceeded due to high admission volume or reduced access to other services. The triage level assigned using the CTAS criteria is a mandatory data element used in almost all Canadian hospital EDs for reporting to CIHI. It has been shown to be valid and reliable, especially when applied by experienced nurses and using electronic decision support tools.
Transition Tracking Tool (T3)
The team has developed a draft Transition Tracking Tool (T3) that we will refine in Phases I and II of the project (described in the next section). We will use it to obtain case related data about individual nursing home residents to track the processes, events and communications among healthcare providers85 in their transition experience, beginning with the decision to transfer from nursing home to ED and ending with the return of the resident to the nursing home or admission to hospital (understanding that some of these persons will die in hospital). The current draft, will be pilot tested in Phase 1, and incorporates the following elements:
-
Nursing home: Demographic and medical data (including medications), reason(s) for transfer, information about the decision and timing of transfer, accompanying documentation during resident transfer from EMS and ED, an assessment of handover communication between nursing home and EMS, and between nursing home and ED not captured in other documentation;
-
EMS: CTAS scores, an assessment of documentation received from nursing home, and prepared or received for ED use, timing of notification that a resident requires transfer (notification and actual transfer times, arrival at ED), an assessment of handover communication between nursing home and EMS not captured in the documentation;
-
Emergency department: Time of arrival, time of placement, time of ED physician assessment, time of consultation, time of disposition, investigations, diagnostic lists, reason for admission, overall length of ED stay (sub-divided into admitted and discharged patients);
-
Disposition: Tracking of the location of the resident following each transfer;
-
Discharge from emergency department to EMS:adequacy of communication between ED and EMS, accompanying documentation with the resident during transfer, timing of notification of and actual transfer; and,
-
Return to nursing home: medical data from ED, accompanying documentation during resident transfer from EMS and ED, assessment of communication at handover.
Older Persons' Transitions in Care Success (OPTICS) Tool
Little attention has been devoted to developing measures that could address the quality of care transitions from NHs to EDs. One such instrument, Coleman's Care Transitions Measure tool, has been used to measure performance around transitions primarily focusing on identifying care deficiencies and approaches to address these deficiencies. It is a self-report tool whose only use has been reported with community based participants. As such it is not appropriate for residents in NHs with dementia or acute confusion. Saliba et al developed a structured implicit review form for use by physicians undertaking retrospective chart audit. This type of tool is useful for research purposes but is less applicable to the needs of decision-makers and managers who need data for quality management. Members of our research team have previously constructed instruments to measure contextual factors in nursing homes that influence care outcomes. In that work we established two criteria for such a measure: (1) feasibility (brevity and ease of completion; the instrument can be completed in 10-15 minutes), and (2) modifiability (focus on concepts that are potentially modifiable). We will apply these criteria when we develop the OPTICS tool to measure success of residents' care transitions.